
Blended Treatment Approach for Recurring C.Difficile Infection
Emily Wolbers
Introduction
Clostridioides difficile infection (CDI) is a diarrheal illness caused by the anaerobic, spore-forming bacillus C. difficile. It is the leading cause of healthcare-associated infectious diarrhea worldwide. There are significantly varying CDI prevalence rates reported globally, with the highest incidence in North America, particularly the United States. The CDC reports 250,000 infections with C.difficile per year and 14,000 deaths annually.¹ These infections impose a burden on the healthcare system, prolonging hospital stays by several days and pose a risk of life-threatening complications, including toxic megacolon, bowel perforation, and sepsis.⁵ Although CDI is historically considered to be a primarily a nosocomial disease, CDC data suggest that roughly half of U.S. cases are community-associated.² Major risk factors include recent antibiotic use, hospitalization or long-term care residence, advanced age, and presence of comorbidities.³
The pathogenesis of CDI is driven by potent bacterial toxins. C. difficile produces two main exotoxins (TcdA and TcdB) and in some strains, the binary toxin CDT. These actions trigger intense mucosal inflammation with cytokine release, resulting in watery diarrhea and abdominal cramping.² Recurrent C.difficile infections are quite common and occur in an estimated 15–35% of treated patients.⁴ Recurrence is defined by a relapse in CDI symptoms within 2-8 weeks of successful treatment.
Given its high morbidity, mortality, and healthcare cost, CDI is classified as an urgent public health threat. The frequent recurrence with pharmacologic interventions underscore the challenges of managing this infection. This case paper aims to demonstrate the clinical utility and efficacy of a combined therapeutic strategy utilizing fecal microbiota transplantation alongside biofilm disruption.
Presenting Concerns
The subject of this case report is a 64-year-old Caucasian male who presented to the clinic with a past medical history significant for CDI. He was previously treated with two courses of oral vancomycin 125 mg every 6 hours for 10 days, without durable resolution of symptoms. He was subsequently prescribed fidaxomicin 200 mg twice daily for 10 days, which resulted in symptom remission for approximately 2 months. Upon recurrence of diarrhea, he was prescribed cholestyramine 4g suspension once daily for symptomatic management.
At the time of consultation, the patient reported 15–16 bowel movements per day, Bristol Stool Scale type 7. He had significant impairment in his ability to perform occupational duties and reported social distress due to abdominal pain and fear of bowel incontinence. His diet was very limited and his appetite was significantly reduced. He was following a strict low FODMAP, lactose-free, gluten-free eating pattern.
Clinical Findings
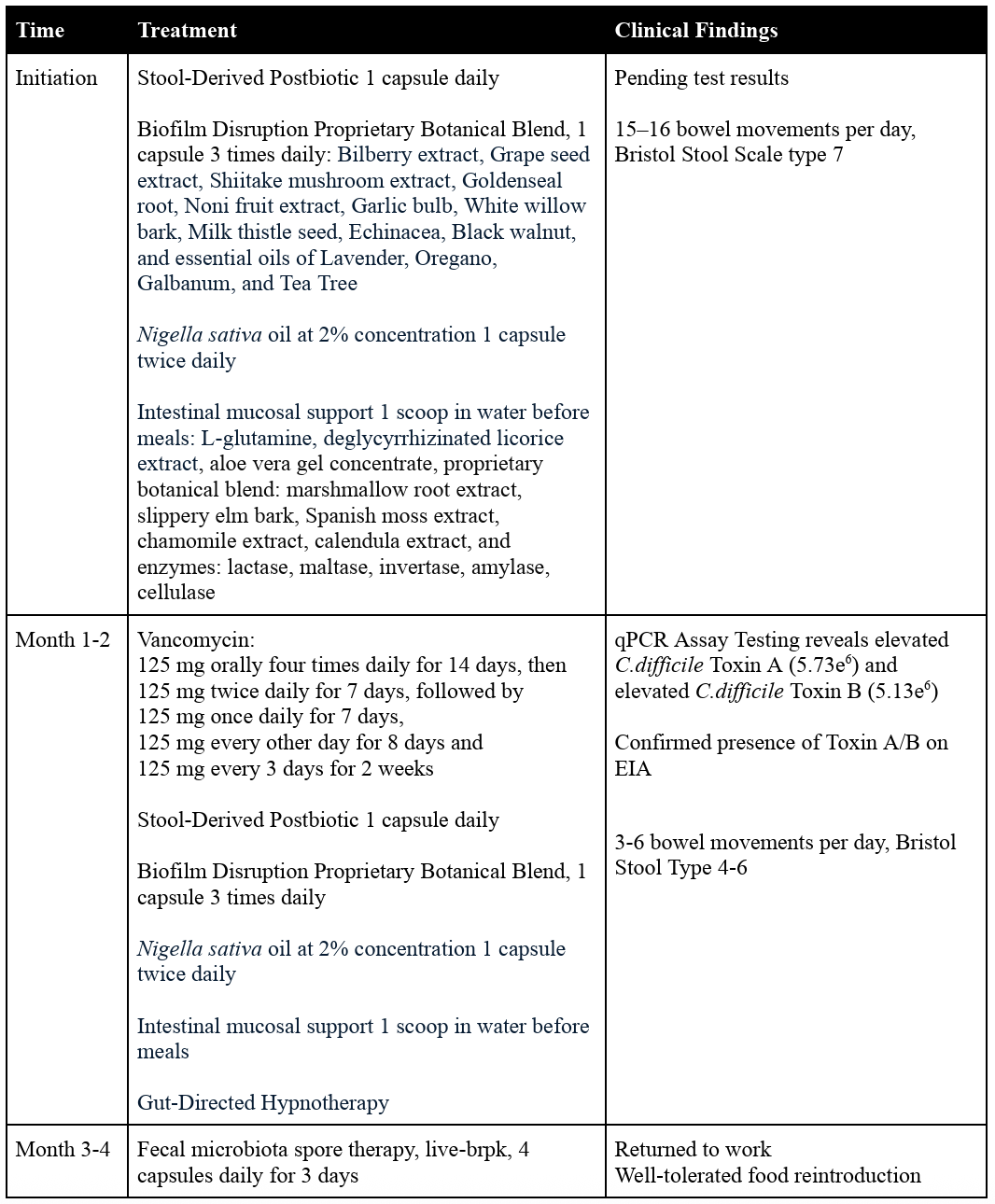
A stool sample was collected after initial consultation. Given his medical history, treatment was initiated prior to receipt of test results to provide symptomatic relief and promote microbiome modulation. Initial treatment consisted of a human stool-derived postbiotic, administered as one capsule daily with meals for 90 days. Concurrently, a biofilm disruption protocol was implemented, consisting of a proprietary botanical blend (see Table 1) at a dose of one capsule three times daily on an empty stomach, along with Nigella sativa oil, one capsule twice daily.¹⁶,¹⁷,¹⁸ Additional powdered supplementation targeting intestinal mucosal support was provided with meals (Table 1).
Initial testing via qPCR assay demonstrated elevated levels of C. difficile toxin A (5.73 × 10⁶) and toxin B (5.13 × 10⁶). Normal reference range < 1.00e³ for C. difficile toxin A and B respectively. Confirmed positive test with stool toxin enzyme immunoassay (EIA). The patient expressed amenability to fecal microbiota transplant and preferred an FDA-approved option. Enrollment for fecal microbiota spore therapy, live-brpk, was initiated, and a vancomycin taper was initiated as follows: 125 mg orally four times daily for 14 days, then 125 mg twice daily for 7 days, followed by 125 mg once daily for 7 days, 125 mg every other day for 8 days (4 doses), and finally 125 mg every 3 days for 2 weeks (5 doses).
During this phase of treatment, the patient was implementing human stool-derived postbiotic, botanical biofilm disruption, Nigella sativa, powdered intestinal mucosal support, and Vancomycin daily. The patient had improved bowel regularity, with 5–6 bowel movements per day, Bristol Stool Scale type 5-6. He was experiencing mealtime anxiety, so additional support with gut-directed hypnotherapy was added to his treatment plan, alongside continued postbiotic therapy, biofilm disruption, and mealtime intestinal support.
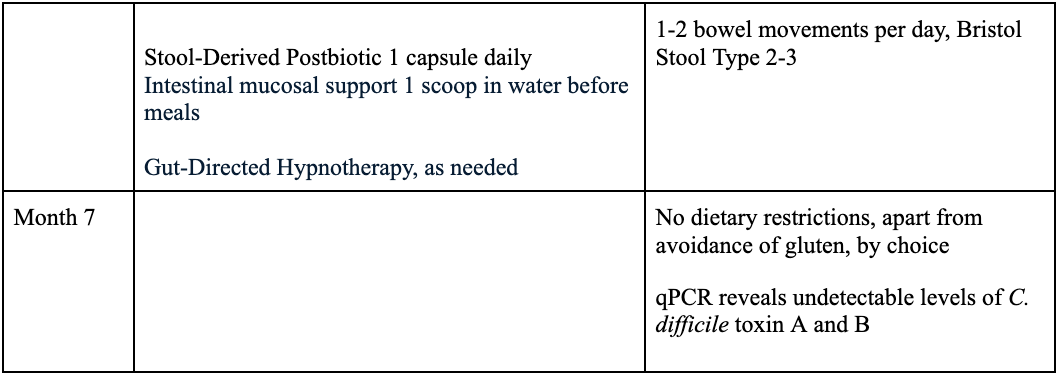
Two months after initiating postbiotic, biofilm disruption, and intestinal support and 4 weeks into his vancomycin taper, the patient began tapering the biofilm disruption protocol. He had returned to work and was able to perform normal occupational duties. Bowel pattern improved to 4-5 bowel movements per day, Bristol Stool type 3-4. Dietary expansion was initiated, with reintroduction of one new food every 2–3 days. He was additionally approved for fecal microbiota spore therapy, which was initiated following completion of vancomycin. Dosing began with 296 mL of magnesium citrate on the day before his first dose of fecal microbiota spores. Fecal microbiota spore therapy was continued with four capsules daily for 3 days.
At the end of treatment, the patient was asymptomatic, with resolution of diarrhea and abdominal pain and improved appetite. He had successfully reintroduced FODMAPs and dairy without adverse effects, while continuing to avoid gluten by preference. The patient continued stool-derived postbiotic therapy during this period, administered as one capsule daily with meals for a total duration of 180 days.
Seven months after his initial consultation, follow-up qPCR testing revealed undetectable levels of C. difficile toxin A and B. At the ten-month follow-up, the patient is still asymptomatic and is able to travel with his family.
Timeline
Table 1: Timeline of Patient Concerns and Interventions
Diagnostic Criteria and Assessment
CDI typically presents as new-onset diarrhea, usually ≥3 unformed, watery stools per 24 hours, often with abdominal pain, abdominal cramping, fever, and loss of appetite. In some cases, CDI may present with ileus with little or no diarrheal symptoms. These patients are often critically ill, with colonic distension and thickening, fever, and leukocytosis. Although this presentation may initially appear mild, it can progress rapidly to severe disease. Diagnosis requires compatible symptoms plus laboratory confirmation of C. difficile. A diagnosis is confirmed by a positive stool test for C. difficile toxin or by endoscopic/histologic evidence of pseudomembranes.⁵
Recurrent CDI (rCDI) is characterized by an initial resolution of symptoms during appropriate treatment, followed by the return of symptoms within two to eight weeks after therapy is discontinued. Approximately 25% of patients experience a recurrence within 30 days of completing treatment, while a smaller proportion may relapse two months later. Patients who develop one recurrence are at substantially higher risk of experiencing additional episodes.⁶
Table 2: Signs and Symptoms of CDI⁵
Symptoms
Acute diarrhea (≥3 loose stools in 24 hours)
Relevant risk factors
Current or recent antibiotic use
Recent hospitalization or long-term care residence
Advanced age
Laboratory Findings
Elevated white blood cell count of up to 15,000 cells/microL
Severe infection may present with
Hypoalbuminemia
Elevated creatinine concentration
Leukocytosis (white blood cell count ≥40,000 cells/microL)
Radiographic Findings
Pseudomembranous colitis on endoscopy is a hallmark finding in CDI
Specimen Collection
For suspected CDI with diarrhea, a two-tiered test is preferred, utilizing a sensitive test glutamate dehydrogenase (GDH) or nucleic acid amplification testing (NAAT) followed by a specific test (Toxin A/B via enzyme immunoassay)
Patients with ileus and suspected CDI, rectal swab collection with GDH, EIA toxin assays, NAAT, or anaerobic culture may be performed
This patient presented with diarrhea within two months of completing antibiotic therapy for CDI, which raises suspicion for recurrent infection. Testing performed with NAAT testing via qPCR resulted positive for C.difficile and was confirmed positive on EIA toxin assay.
Following treatment, there is no indication to test for cure in CDI, and there is also no indication for repeat testing in asymptomatic patients.⁵ Per patient request, a post-treatment qPCR test was performed.
Therapeutic Interventions
Antibiotics
Antibiotic use is the primary risk factor for developing CDI, and yet antibiotics are still the standard first line treatment option for C.difficile infections. Vancomycin and fidaxomicin are the recommended antibiotics for primary and recurring CDI. However, C.difficile spores can survive antimicrobial therapy, and a relapse of CDI can occur after germination.⁷ For patients seeking alternative treatment, a course of vancomycin or fidaxomicin is part of the inclusion criteria to be considered for FDA-approved Fecal Microbiota Transplant (FMT).⁸ This paper explores a blended approach to care utilizing microbiome restoration.
Fecal Microbiotia Transplant
Studies are consistent that FMT is the most effective approach to CDI to restore the gut microbiome and reduce colonization by pathogenic organisms. FMT has demonstrated high efficacy in preventing rCDI, particularly in patients with multiple recurrences, with many studies reporting cure rates exceeding 90%.⁹ Advances in FMT delivery have included the use of frozen stool preparations, the establishment of stool banks, and the development of more patient-friendly formulations such as lyophilized oral capsules.
The process of FMT consists of stool collection from a healthy individual. The donor’s fecal bacteria and microbes are transferred into an infected patient to replenish healthy gut microbiota. Studies comparing delivery methods have shown that colonoscopy, nasoduodenal tube, and oral capsules all have comparable efficacy.¹⁰ A colonoscopic method of delivery induced marginally more adverse events, including abdominal pain, bloating, and diarrhea, but had the benefit of direct view of the intestinal lining. Nasoduodenal delivery had the highest degree of inconsistency in between studies, likely due to procedural variables. Oral capsules were shown to be most preferred by patients.¹⁰
There are FDA-approved microbiome-based therapies, approved for prevention of recurring CDI. At the time of this paper there are Vowst™ (fecal microbiota spores, live-brpk) and Rebyota™ (fecal microbiota, live-jslm). Vowst™ is an oral live biotherapeutic product, while Rebyota™ is a single-dose rectal suspension.¹¹, ¹² While these live biotherapuetic products (LBPs) are highly standardized, they come with drawbacks, which are elucidated in the discussion section.
Postbiotics
Postbiotics are an emerging therapy for combating antibiotic resistance. Postbiotics are bioactive metabolites that are produced as a byproduct from the action of probiotics. They are known to enhance host immune function, strengthen intestinal barrier function, and influence microbial composition, which makes them an allied therapy in many disease processes. In CDI, postbiotics have a complex method of action. Postbiotics directly inhibit the growth of C. difficile and hinder its ability to produce toxins by affecting the formation of biofilms and altering gene expression.¹³
Postbiotic therapy in populations with underdeveloped or disrupted microbiota, such as premature infants, has been associated with decreased inflammation, improved digestive function, and overall health support.¹⁴ They may also have therapeutic potential in recurrent infection by helping restore microbiome stability.¹⁴ Though additional studies are needed, postbiotics represent a promising adjunctive approach in CDI management and in antimicrobial resistance.
Biofilms
Biofilms are structured formations that act as a protective matrix and a reservoir for bacteria to survive treatments. The complexity of biofilm physiology and the difficulty of delineating biofilm-associated bacteria from luminal bacteria has made studying biofilms in rCDI challenging.
Early studies show that in vitro, C. difficile can embed itself within the colonic biofilm community, and once embedded, it becomes much more resilient to vancomycin, and even FMT. This may help explain the prevalence of rCDI even after therapy seems successful.¹⁵
There are numerous naturally occurring biofilm-disrupting agents that degrade protective microbial matrices. Research on herbs, plant-based phytochemicals, enzymes, and other compounds targeting biofilm disruption is extensive and continues to expand, driven in part by the rising prevalence of multidrug-resistant infections.¹⁶ For example, studies on Nigella sativa oil at 2% concentration has been shown to inhibit growth of several both Gram-positive and Gram-negative bacteria, including C.difficile.¹⁷, ¹⁸ The botanical biofilm disruption blend used for this patient has been studied for its efficacy against biofilm-associated infections, namely Staphylococcus aureus, Pseudomonas aeruginosa, Klebsiella pneumoniae,and Candida albicans. In vitro studies show that concentrated dosing resulted in biofilm eradication of P. aeruginosa, S. aureus, and E. coli.¹⁹ Further investigation into the effects of herbal biofilm disruptors on C. difficile is warranted. Current evidence has limited research on botanical biofilm disruption and remains largely limited to in vitro studies.
Discussion
In patients with recurrent diarrhea and a prior diagnosis of CDI, it can be challenging to determine whether a positive NAAT or GDH result reflects active infection or persistence from a previous episode. In this case, clinical assessment guided the decision to initiate treatment. FMT demonstrates the highest overall efficacy in rCDI, with cure rates commonly reported >80–90%.⁹ Over time, FMT has evolved to include more modern delivery methods. Initially administered as a fecal slurry for oral consumption, it progressed to rectal enemas and, more recently, encapsulated formulations. This evolution has improved both accessibility and patient acceptability.²⁰ Stool banks have further expanded access; however, since 2023, the regulatory landscape in the United States has shifted, with FMT now subject to FDA oversight.
FDA-approved microbiota-based therapies offer standardized and clinically validated alternatives, though limitations remain. Vowst™ has demonstrated significant reduction in recurrence at eight weeks, with durable response at 6 months, but is designed to restore spore-forming Firmicutes rather than full microbiome diversity. Rebyota™ demonstrated a 70.6% success rate at eight weeks, with sustained response in >90% of initial responders at six months.²¹ While both therapies provide improved standardization and safety, access may be limited by strict eligibility criteria and high cost, with treatment ranging from approximately $9,500 to $17,500 compared to $500–$1,500 for traditional FMT.
In this case, a multimodal approach incorporating fecal microbiota transplantation, biofilm disruption, and postbiotic therapy was associated with sustained clinical remission and microbiologic clearance. While FMT alone has demonstrated high efficacy in rCDI, this case highlights the potential benefit of addressing additional pathogenic mechanisms, including biofilm persistence and impaired microbiome resilience. The integration of adjunctive therapies may enhance treatment durability and reduce recurrence risk, particularly in patients with a history of refractory or recurrent disease. Although these findings are promising, further clinical investigation is warranted to evaluate the efficacy and generalizability of combined therapeutic strategies in the management of rCDI.
References
Akorful RAA, Odoom A, Awere-Duodu A, Donkor ES. The global burden of Clostridioides difficile infections, 2016–2024: a systematic review and meta-analysis. Infect Dis Rep. 2025;17(2):31. doi:10.3390/idr17020031
Smits WK, Lyras D, Lacy DB, Wilcox MH, Kuijper EJ. Clostridium difficile infection. Nat Rev Dis Primers. 2016;2:16020. doi:10.1038/nrdp.2016.20
Eze P, Balsells E, Kyaw MH, Nair H. Risk factors for Clostridium difficile infections: an overview of the evidence base and challenges in data synthesis. J Glob Health. 2017;7(1):010417. doi:10.7189/jogh.07.010417
Singh T, Bedi P, Bumrah K, et al. Updates in treatment of recurrent Clostridium difficile infection. J Clin Med Res. 2019;11(7):465-471. doi:10.14740/jocmr3854
Kelly CP, Lamont JT. Clostridioides difficile infection in adults: clinical manifestations and diagnosis. UpToDate. Updated 2025. Accessed April 17, 2026.
McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin Infect Dis. 2018;66(7):e1-e48. doi:10.1093/cid/cix1085
Bishop EJ, Tiruvoipati R. Management of Clostridioides difficile infection in adults and challenges in clinical practice: review and comparison of current IDSA/SHEA, ESCMID and ASID guidelines. J Antimicrob Chemother. 2023;78(1):21-30. doi:10.1093/jac/dkac404
US Department of Veterans Affairs Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Fecal microbiota spores, live-brpk (Vowst): criteria for use. Published March 1, 2025. Updated February 2025. Accessed April 15, 2026.
Chapman BC, Moore HB, Overbey DM, et al. Fecal microbiota transplant in patients with Clostridium difficile infection: a systematic review. J Trauma Acute Care Surg. 2016;81(4):756-764. doi:10.1097/TA.0000000000001195
Ray R, Hack SA, Vij AK, et al. Efficacy of fecal microbiota transplantation versus standard antibiotic therapy in recurrent Clostridioides difficile infection: a systematic review and meta-analysis. Cureus. 2025;17(8):e90614. doi:10.7759/cureus.90614
Reigadas E, van Prehn J, Falcone M, et al. Prophylactic interventions for prevention of Clostridioides difficile infection. Clin Microbiol Infect. 2021;27(12):1777-1783. doi:10.1016/j.cmi.2021.06.037
Blair HA. SER-109 (Vowst): a review in the prevention of recurrent Clostridioides difficile infection. Drugs. 2024;84(3):329-336. doi:10.1007/s40265-024-02006-7
Asghari Ozma M, Mahmoodzadeh Hosseini H, Ataee MH, Mirhosseini SA. Evaluating the antibacterial, antibiofilm, and antitoxigenic effects of postbiotics from lactic acid bacteria on Clostridioides difficile. Iran J Microbiol. 2024;16(4):497-508. doi:10.18502/ijm.v16i4.16309
Singh C, Singh A, Singh D, Upadhyay R. Potential therapeutic solution for Clostridioides difficile infection: current scenario and future prospects. Med Microecol. 2025;24:100121. doi:10.1016/j.medmic.2025.100121
Normington C, Moura IB, Bryant JA, et al. Biofilms harbour Clostridioides difficile, serving as a reservoir for recurrent infection. npj Biofilms Microbiomes. 2021;7(1):16. doi:10.1038/s41522-021-00184-w
Shamim A, Ali A, Iqbal Z, et al. Natural medicine a promising candidate in combating microbial biofilm. Antibiotics (Basel). 2023;12(2):299. doi:10.3390/antibiotics12020299
Aljarallah KM. Conventional and alternative treatment approaches for Clostridium difficile infection. Int J Health Sci (Qassim). 2017;11(1):1-10.
Hanafy MSM, Hatem ME. Studies on the antimicrobial activity of Nigella sativa seed (black cumin). J Ethnopharmacol. 1991;34(2-3):275-278. doi:10.1016/0378-8741(91)90047-H
Mundanchira AV, Wong A, Klos-Maki K, Strand J, Marques CNH. Activity of Biocidin® against microbial biofilms. Front Antibiot. 2026;4:1692653. doi:10.3389/frabi.2025.1692653
Barron M. Fecal microbiota transplants (FMT): past, present and future. American Society for Microbiology. Published June 10, 2025. Accessed April 17, 2026.
Lee A, Yoo JS, Yoon EJ. Gut microbiota and new microbiome-targeted drugs for Clostridioides difficile infections. Antibiotics. 2024;13(10):995. doi:10.3390/antibiotics13100995